
The second day of Cure‘s “The Power of X” summit concluded yesterday, with a shift from market analysis to implementation. While day one established the scale of opportunity – a $1 trillion women’s health market receiving just 2% of healthcare venture funding – day two tackled the barriers preventing this potential from being realized.
Throughout the discussions, a clear message emerged: Transforming women’s health requires changes across the entire healthcare ecosystem – from research and technology to funding structures, care delivery, and reimbursement systems. Speakers not only identified these challenges but presented tested strategies and actionable frameworks for moving forward.
Breaking the Self-Reinforcing Cycle
The day’s conversations revealed a troubling cycle hampering women’s health innovation. Research gaps create care gaps, which lead to reimbursement gaps, which then reinforce research gaps. Breaking this pattern requires coordinated action at multiple points.
Former NBC Today Show correspondent Kristen Dahlgren showed how this disruption can begin with personal advocacy. Following her 2019 breast cancer diagnosis, Dahlgren founded the Cancer Vaccine Coalition to accelerate promising vaccines already in clinical trials.
“We spend $29 billion every year on breast cancer care. For about a billion dollars, we can have these vaccines to market,” Dahlgren explained. “We are going through these barbaric and outdated treatments when there is better science ahead.”
TV personality Stacy London described a similar disconnect in menopause care: “When I started talking about it in 2018, people told me I was committing career suicide.” Now, with a billion people in menopause worldwide, the market opportunity is clear – yet the funding-to-market pipeline remains underdeveloped.
Data as the Essential Foundation
A consistent message across presentations was the importance of sex-specific data collection and analysis. The historical exclusion of women from clinical trials has created knowledge gaps about how diseases manifest and how treatments work in women’s bodies.
Several speakers highlighted autoimmune disorders as a prime example of this data deficit. Dr. Sonia Sharma of La Jolla Institute for Immunology noted that “75 to 80% of people who are afflicted with autoimmune disease today are women,” yet research is hampered by the unpredictable nature of these conditions and lack of longitudinal studies.
“We do this for cardiovascular disease. Why can’t we do this for autoimmunity?” asked Dr. Rekha Kumar of Weill Cornell Medicine, pointing out that data collection methods proven effective in male-predominant conditions haven’t been applied to female-predominant ones.
New technologies are beginning to address these gaps. Dr. Pita Navarro, Chief Scientific Officer at Evvy, described how advanced sequencing techniques are transforming vaginal microbiome testing, replacing subjective diagnoses with data-driven approaches. This has led to much better outcomes and increased willingness among women to contribute to research.
But data collection alone isn’t sufficient. Linda Blount, President of the Black Women’s Health Imperative, is developing a tool that analyzes documentation, protocols, and implementation plans to identify and combat bias in existing data and healthcare delivery systems.



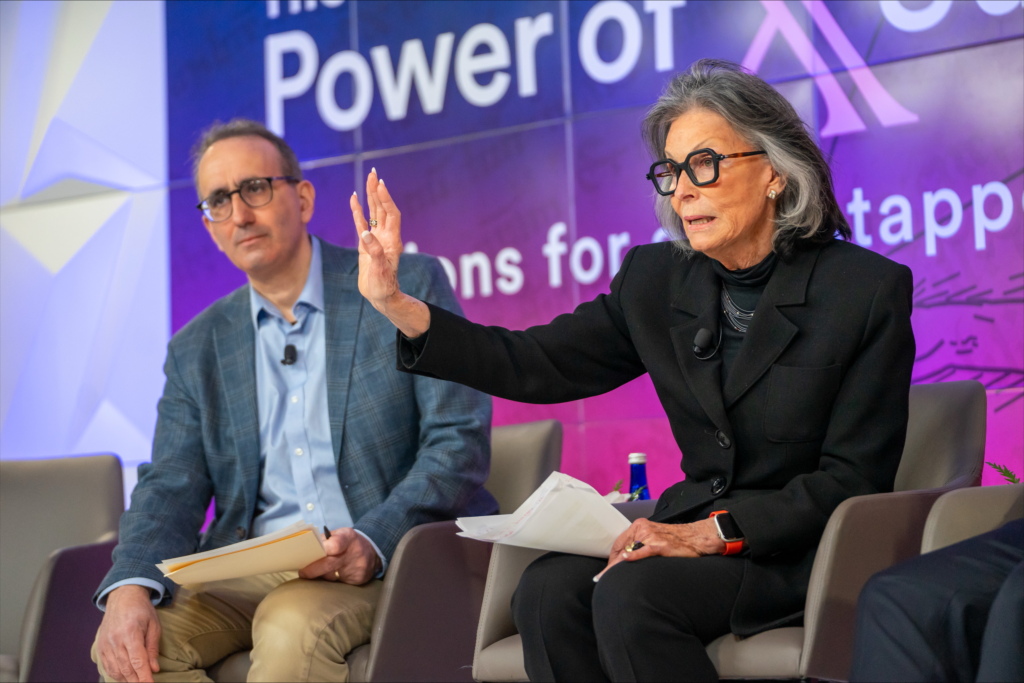
Images: Cure
Representation and Accessibility: Essential Twin Pillars
The statistics shared during the summit underscored why representation matters: “Black women are three or four times more likely to die during pregnancy or as a result of pregnancy,” while “22% of Latinas are uninsured in this country.”
Blount emphasized that these disparities stem from system design, not biology: “The systems of healthcare delivery, research and development, and bringing therapeutics to market are designed to benefit the people who created them. There’s no biological determinant for race, so it can’t explain the disparities we see.”
New approaches to expanding access are emerging. Dr. Reggie Swift described retrofitting Chevy Suburbans with x-ray machines in Africa, a decentralized care model now being adapted for U.S. communities. Julie Campbell of Mercer highlighted employer-driven innovations like in-bra lactation devices that allow women to “not leave the meeting… they can be present while they continue to nourish their child.”
However, speakers also emphasized that individual technologies can’t overcome systematic barriers to access. Reimbursement reform emerged as perhaps the most fundamental need, with In Women’s Health’s Jodi Neuhauser noting that of 10,000 CPT codes in the United States, “less than 5% have anything to do with women’s health.”
Paloma Health Co-founder Marina Tarasova cited research identifying approximately 2,000 procedures where “when you compare apples to apples… the male procedure will be reimbursed 30% higher.” This translates directly to care quality, as OB-GYNs need to “see upwards of 30 patients in a day to keep the lights on,” leaving just seven minutes per patient.
Collaborative Models: Building a New Ecosystem
Despite these challenges, the summit showed encouraging trends in new funding and collaboration models specifically designed for women’s health.
Rachel Butler, President of the Catalytic Impact Foundation, explained their approach to early-stage funding gaps: “We aggregate philanthropic capital, pool it, and then run it as an early stage venture fund.” This allows the organization to support companies with “a little more risk, go in a little earlier, and have longer time frames” than traditional venture investment.
To overcome market fragmentation, Marina Tarasova described the Wonder Woman Collective, where specialized women’s health companies “have come together to approach payers and brokers and large employers as a one-stop shop,” making comprehensive solutions easier to implement.
Ayodola Anise announced the Milken Institute‘s upcoming Women’s Health Network, launching in May 2025. The new platform aims to connect “patient and advocacy organizations, researchers, investors, academic organizations, health systems and policy makers” to amplify existing work and create new connections between researchers and investors.
Throughout the summit, speakers emphasized the power of community in driving change. Stacy London, who transitioned from fashion expert to midlife health advocate, introduced the concept of an “enchantress archetype” – a stage between the traditional female archetypes of mother and elder. As London explained, the enchantress represents midlife women who use their experience and wisdom to build communities – just like the many women present at the conference do day in, day out: “It’s about creating community – finding your people, finding the people who are going to rally behind you to challenge and change the status quo.”
The inaugural “Power of X” Summit” concluded with consensus: Transforming women’s health requires action across the ecosystem – from research and data collection to funding models, care delivery, and policy. Through strategic collaboration, the $1 trillion women’s health opportunity represents not just a market, but a revolution in care that is now no longer out of reach.

